From the blog
Another Autumn, Another COVID Jab. Or not?
In the United States, the CDC recommends the new COVID booster for everyone over the age of 6 months. In most of Europe, including Germany, France, Italy, and the UK, that same booster is only recommended for people over the age of 65 or f
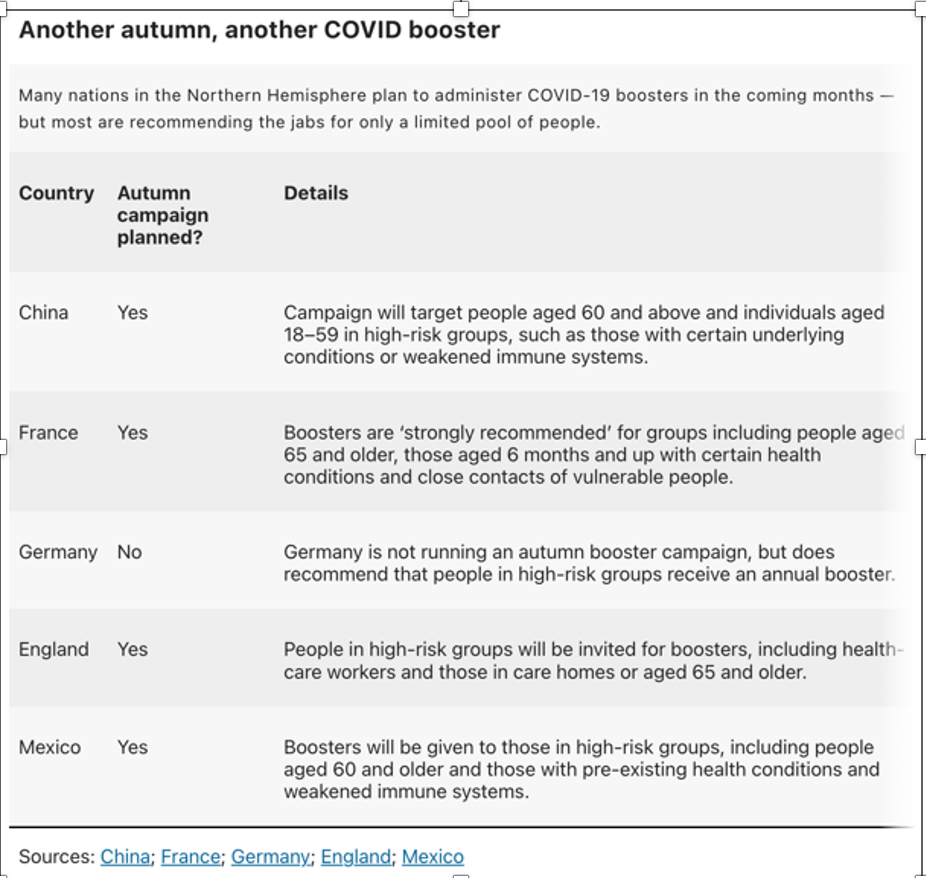
In the United States, the CDC recommends the new COVID booster for everyone over the age of 6 months. In most of Europe, including Germany, France, Italy, and the UK, that same booster is only recommended for people over the age of 65 or for younger people who are in high risk groups (including health professionals). Israel, which was a strong proponent of vaccines in 2021, has yet to issue any recommendations for this fall. Critics of the new vaccine claim that there just aren’t any high-quality randomized trials showing safety and efficacy. European policies split the difference. American policies double-down on the pro-vaccine approach.
Why the difference? If the benefits of immunization clearly outweigh the risks, then scientists, economists, and public health officials in different countries should come to similar conclusions and recommendations. But the known benefits differ in different age groups. European countries justify their recommendations by arguing that COVID is usually mild in young healthy people, and that, since most young healthy people have already had the disease or been immunized or both, they are already protected. In the US, many scientists say that younger people who are healthy and already vaccinated will still have some protection against severe disease if they sit out this round of jabs. But they also say that even for individuals not in high-risk groups, a booster would reduce the risk of a new SARS-CoV-2 infection — albeit fleetingly — and offer other advantages, too. “Anyone who takes it will benefit,” says immunologist Rafi Ahmed at Emory University in Atlanta, Georgia.
The CDC justified its recommendations by comparing morbidity and mortality from COVID to that associated with other vaccine preventable diseases. They showed that, among unimmunized children, death rates were much higher for COVID than for hepatitis A, Varicella, Rubella, and Rotavirus. Thus, they argue, if we recommend vaccines for those other diseases, we should recommend them to prevent COVID. Of note, in many European countries, children are not routinely immunized against rotavirus, hepatitis A, or varicella.
Epidemiologist Katelyn Jetelina makes a different argument for why the US is an outlier and why that is not a bad thing. She suggests that, here in the US, we need more vaccines because our health care system is so bad. “U.S. healthcare is hard to access, has poor administrative efficiency, and lacks equity. This means that if someone gets sick, it’s hard to get help. And, as we’ve seen throughout the pandemic, it’s harder for certain groups than others. This means we need to do even more in the U.S. to prevent infectious diseases and their poor outcomes, including hospitalization and death, than in other high-income countries. In addition, the US doesn’t have paid sick leave, it has a higher proportion of people over 65 in the work force, more people living in poverty, and more people with chronic health conditions.
There is another quirk in the US health care system, compared to those in Europe. Once the CDC recommends a vaccine, insurers cover the costs. Thus, a recommendation allows access to vaccines. In most European countries, access is determined by the same governmental entities that pay for health care. They don’t rely, as we do, on private insurance or separate public programs such as Vaccines for Children.
In other words, as with so many other aspects of our health care system, the administrative complexity adds costs, decreases quality, and leads to inefficiencies and irrationalities that make it difficult to provide high quality care.
I will get the vaccine. I am a health care worker over the age of 65, so I would be eligible both here and in European countries with more restrictive policies. With parents, I will discuss the pros and cons. I will talk about what we know about benefits and risks and about the limitations of our knowledge. I suspect that most parents will decline. After all, only 13% of children under 5 in the US have gotten even one dose of prior COVID vaccines. I just hope that our confused and confusing policies do not shake parents’ faith in other vaccines. Some evidence suggests that is already occurring, both in the US and around the world.
Related writing.
Why the Dutch Keep Pediatric Euthanasia Illegal
Pediatric euthanasia in The Netherlands has a unique legal status - it is illegal, openly practiced, and well-regulated. The most surprising part isn't the law that enabled this — it's what happened after.
The Lost Aura of the Doctor in the Age of AI
	Artificial intelligence can now make difficult diagnoses, detect drug interactions, read medical images, predict outcomes, counsel patients — and even write peer reviews. As these capabilities expand, doctors risk becoming supervisors
The Tiniest Patients: Rethinking How We Decide
	When a baby is born at 22 or 23 weeks of pregnancy — half the normal gestational period — doctors and parents face one of the most agonizing decisions in all of medicine. Should they fight to keep the baby alive, knowing survival is u
Emilia Perez: New Life or New Gender?
The award-winning film Emilia Perez addresses a central question in gender medicine. When a patient wants to transition, is it because they want to change their gender or because they want to change their life? If the later, a gender trans
About the author
John D. Lantos is a pediatrician and bioethicist writing on AI in medicine, neonatal intensive care, and end-of-life decisions. His essays appear in JAMA, JAMA Pediatrics, the Hastings Center Report, the New England Journal of Medicine, and Aeon. Read more about John.